Urinary Stone
» A kidney stone, also known as a renal calculus (from the Latin rēnēs, “kidneys,” and calculus, “pebble”), is a solid concretion or crystal aggregation formed in the kidneys from dietary minerals in the urine.
» Urolithiasis (UL) is one of the most common diseases, with approximately 7.6% incidence in Western India. Although most patients have only one stone episode, 25% of patients experience recurrent stone formation. UL therefore has a significant impact on quality of life and socioeconomic factors.
» Urinary stones are typically classified by their location in the kidney (nephrolithiasis), ureter(ureterolithiasis), or bladder (cystolithiasis), or by their chemical composition (calcium-containing, struvite, uric acid, or other compounds).
» About 60-80% of those with kidney stones are men.
» Urinary stones are highly prevalent in Madhya Pradesh and neighbouring states like Gujarat and Rajasthan due to the hot and humid climate, poor water intake and urinary infections. Patients routinely get pain in the flanks, vomiting, burning while passing urine. Occasionally they also get fever and blood in the urine.
» Two very important facts to be noted are:
1. 20% of urinary stone patients do not have any complaints and hence are detected in screening or health check up programs.
2. 3% of patients with kidney stones present with kidney failure.
» Sonography is the best and the most routine test performed to detect urinary stones. Blood and urine tests along with X-ray test are also required.
» The existence of kidney stones was first recorded thousands of years ago, and lithotomy for the removal of urinary stones is one of the earliest known surgical procedures.
» In 1901, a stone discovered in the pelvis of an ancient Egyptian mummy was dated to 4,800 BC.
» Part of the Hippocratic Oath suggests there were practicing surgeons in ancient Greece to whom physicians were to defer for lithotomies. Medical texts from ancient India, Persia, Greece and Rome all mentioned calculous diseases.
» Famous people with kidney stones include Napoleon I, Napoleon III, Peter the Great, Louis XIV, George IV, Oliver Cromwell, Lyndon B. Johnson, Benjamin Franklin, Michel de Montaigne, Isaac Newton, William Harvey, Herman Boerhaave, and Antonio Scarpa.
» New techniques in lithotomy began to emerge starting in 1520, but the operation remained risky.After Henry Jacob Bigelow popularized the technique of litholapaxy in 1878, the mortality rate dropped from about 24% to 2.4%. However, other treatment techniques continued to produce a high level of mortality, especially among inexperienced urologists.
» In 1980, Dornier MedTech introduced extracorporeal shock wave lithotripsy for breaking up stones via acoustical pulses, and this technique has since come into widespread use.
Kidney stones affect all geographical, culture, and racial group.
» The lifetime risk is about 10 to 15% in the developed world, but can be as high as 20 to 25% in the Eastern world. The increased risk of dehydration in hot climates, coupled with a diet 50% lower in calcium and 250% higher in oxalates compared to Western diets, accounts for the higher net risk in the Middle East. In the Middle East, uric acid stones are more common than calcium-containing stones.
» The number of deaths due to kidney stones is estimated at 19,000 per year being fairly consistent between 1990 and 2010.
» In North America and Europe, the annual incidence (number of new cases per year) of kidney stones is roughly 0.5%. In the United States, the prevalence (frequency in the population) of urolithiasis has increased from 3.2% to 5.2% from the mid-1970s to the mid-1990s.
» About 65% of those with kidney stones are men. Men most commonly experience their first episode between 30 and 40 years of age, whereas for women, the age at first presentation is somewhat later. The age of onset shows a bimodal distribution in women, with episodes peaking at 35 and 55 years.
» Recurrence rates are estimated at 50% over a 10-year and 75% over 20-year period, with some people experiencing ten or more episodes over the course of a lifetime.
A majority of kidney stones are calcium stones, with calcium oxalate (CaOx) and calcium phosphate (CaP) accounting for approximately 80% of all of these stones, uric acid (UA) about 9%, and struvite (magnesium ammonium phosphate hexahydrate, from infection by bacteria that possess the enzyme urease) approximately 10%, leaving only 1% for all the rest (cystine, drug stones, ammonium acid urate).
» A total of 1050 urinary calculi (900 renal, 150 ureteric) were analyzed by X-ray diffraction crystallography technique, in patients managed at All India Institute of Medical Sciences. The stone fragments were collected after extracorporeal shock-wave lithotripsy, or retrieval by endoscopic (percutaneous nephrolithotomy, ureterorenoscopy), laparoscopic and various open surgical procedures. The structural analysis of the stones was done using X-ray diffraction crystallography.
» Of the 1050 stones analyzed, 977 (93.04%) were calcium oxalate stones, out of which 80% were calcium oxalate monohydrate (COM) and 20% were calcium oxalate dihydrate (COD). Fifteen were struvite (1.42%) and 19 were apatite (1.80%).Ten were uric acid stones (0.95%) and the remaining 29 (2.76%) were mixed stones (COM + COD and calcium oxalate + uric acid, calcium oxalate + calcium phosphate, and calcium phosphate + magnesium ammonium phosphate).
Urinary stones are typically classified by:
A – Their location in the kidney (nephrolithiasis), ureter (ureterolithiasis),or bladder (cystolithiasis), or
B – Chemical Composition(calcium-containing, strvite, uric acid , or other compounds).
1. Dehydration from low fluid intake is a major factor in stone formation.
2. High dietary intake of animal protein, sodium, refined sugars, fructose, and oxalate, increase the risk of kidney stone formation.
3. Kidney stones can result from an underlying metabolic condition, such as hyperparathyroidism, distal renal tubular acidosis, primary hyperoxaluria, or medullary sponge kidney. 3–20% of people who form kidney stones have medullary sponge kidney.
4. Kidney stones are more common in people with Crohn’s disease. Crohn’s disease is associated with hyperoxaluria and malabsorption of magnesium.
A person with recurrent kidney stones may be screened for such disorders. This is typically done with a 24-hour urine collection. The urine is analyzed for features that promote stone formation.
The Role of Global Warming Epidemiologic studies have shown that regions with higher average temperatures have the highest stone rates. The correlation between increased environmental temperature and increased number of stone events supports the conclusion that global warming has an impact on the development of stones.It has been predicted that, based on the effects of global warming, the percentage of people living in areas designated as high risk for kidney stone formation would increase from 40% in 2000 to 56% by 2050, and up to 70% by 2095. This would result in a significant “climate-related” increase in kidney stone events.
Diagnosis of kidney stones is made on the basis of information obtained from
1. the history,
2. physical examination
3. urinalysis, and
4. radiographic studies.
Clinical diagnosis is usually made on the basis of the location and severity of the pain, which is typically colicky in nature (comes and goes in spasmodic waves). Pain in the back and flank occurs when calculi produce an obstruction in the kidney.
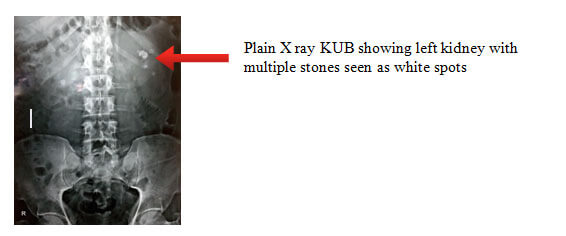
Calcium-containing stones are relatively radiodense, and they can often be detected by a traditional radiograph of the abdomen that includes the kidneys, ureter, and bladder (X Ray KUB film).Some 60% of all renal stones are radiopaque . In general, calcium phosphate stones have the greatest density, followed by calcium oxalate and magnesium ammonium phosphate stones. Cystine calculi are only faintly radiodense, uric acid stones are usually entirely radiolucent ( not seen on X-ray).
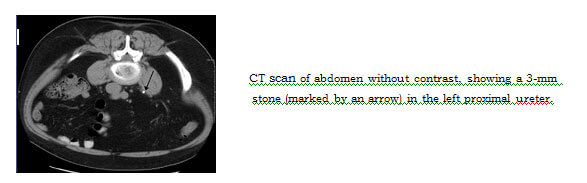
Where available, a CT Scan is the diagnostic modality of choice in the radiographic evaluation of suspected nephrolithiasis. All stones are detectable on CT scans except very rare stones composed of certain drug residues in the urine, such as from indinavir.
Where a CT scan is unavailable, an intravenous pyelogram may be performed to help confirm the diagnosis of urolithiasis. This involves intravenous injection of a contrast agent followed by a KUB film.
Ultrasound imaging the stone is blocking the outflow of urine. Radiolucent stones,which do not appear on KUB, may show up on ultrasound imaging studies. Other advantages of renal ultrasonography include its low cost and absence of radiation exposure. Ultrasound imaging is useful for detecting stones in situations where X-rays or CT scans are discouraged, such as in children or pregnant women.
- Microscopic examination of the urine,which may show red blood cells, bacteria leukocytes,urinary casts and crystals. Also important is the urinary pH.
- Urine culture to identify any infecting organisms present in the urinary tract and sensitivity to determine the susceptibility of these organisms to specific antibiotics;
- Complete blood count(CBC), looking for increase neutrophil count suggestive of bacterial infection, as seen in the setting of struvite stones or any stone with kidney infection;
- Renal function blood test (Creatinine, Urea) to look for loss in renal fuction.
- Blood Test for abnormally high blood calcium blood levels (hypercalcemia);
- 24 hour urine collectionto measure total daily urinary volume, magnesium, sodium, uric acid, calcium, citrate, oxalate and phosphate;
- Chemical analysis os stones:collection of stones (by urinating through a Stone-Screen kidney stone collection cup or a simple tea strainer) is useful. Chemical analysis of collected stones can establish their composition, which in turn can help to guide future preventive and therapeutic management.
Most stones less than 6 mm pass spontaneously.
Increased and regular fluid intake forms the mainstay of treatment. Analgesics (pain killers) are given as and when required.
Medications like alpha blockers (Tamsulosin or Alfuzosin) help in spontaneous passage of small stones.
Surgical or Minimal Invasive Treatment of Urinary Stones
Beginning in the mid-1980s, less invasive treatments such as extracorporeal shock wave lithostripdy and endoscopic surgery began to replace open surgery as the modalities of choice for the surgical management of urolithiasis.
Complete removal of the stone is an important goal in order to eradicate kidney infection, relieve obstruction, prevent further stone growth and associated infection preserve kidney function.
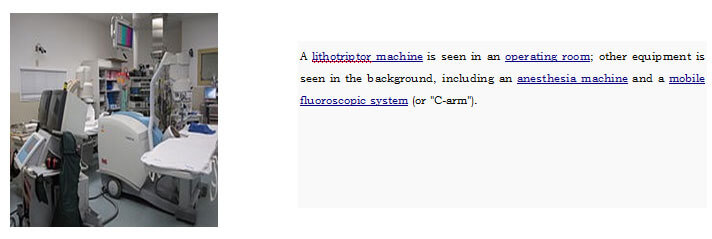
Extracorporeal shock wave lithotripsy (ESWL) is a noninvasive technique for the removal of kidney stones. ESWL involves the use of a lithotriptor machine to deliver externally applied, focused, high-intensity pulses of ultrasonic energy to cause fragmentation of a stone over a period of around 30–60 minutes.
It is currently used in the treatment of uncomplicated stones located in the kidney and upper ureter, provided the aggregate stone burden (stone size and number) is less than 20 mm and the anatomy of the involved kidney is normal.
However due to unpredictable and poor results and need for multiple sessions and procedures, the use of ESWL is on the decline and is being replaced by minimal invasive modalities like Ureteroscopy or PCNL.
Need for endoscopic surgery arises when a patient has:
- Stones larger than 8mm that are unlikely to pass
- only one working kidney with stone,
- bilateral obstructing stones,
- a urinary tract infection or an infected kidney, or intractable pain.
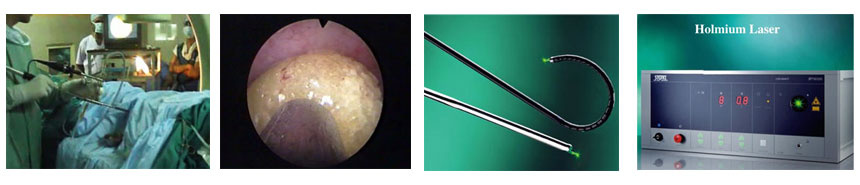
Endoscopic surgery is named as per the location of stone.
- Cystolithotrity: Removal of stones in the urinary bladder.
- Ureteroscopy: Removal of stones in the ureter.
- PCNL( Percutaneous Nephrolithotomy): Removal of the stone in the kidney.This endoscopic surgery offers the highest success rates with regards to complete stone clearance. This is now done using the MiniPCNL 5mm endoscope.
Flexible ureteroscopy (RIRS) with holmium laser has evolved in the last decade to facilitate treat kidney stones unto 1.5cm size.
- The prevalence of urolithiasis in children depends on socioeconomic conditions as well as ethnicity.
- The incidence of urolithiasis has increased worldwide, independent of age.
- Lifestyles changes especially dietary, and the obesity epidemic have been suggested as potential causes.
- In underdeveloped countries, malnutrition is a major reason for the prevalence of bladder stones and ammonium urate stones in children.
- Pediatric urinary stone patients belong to the high-risk group for recurrent urinary stones. As such, these patients and their families need specific therapeutic directions for effective stone prevention, adjusted to their metabolic risk. The risk may be based on anatomic or functional disorders of the urinary collecting system and/or metabolic abnormalities including genetic disorders.
Role of Diet in formation of urinary stone
Recommendations
High Fluid intake is the most important dietary modification to reduce chances of stone recurrence.
- A fluid intake that will achieve a urine volume of at least 2.5 liters daily
- A sufficiently dilute urine will prevent the individual chemical components of stones from becoming concentrated enough to precipitate out of solution, keeping them instead in their dissolved state.
- A high urine output also may reduce stone from forming through “flushing” out of stone components and prevention of urine stagnation.
- In addition to stone benefits, increased water intake has been shown to have a multitude of other benefits, including improved alertness, better skin appearance, enhanced physical performance, reduced constipation.
- Limit sodium intake to less than 2.3gm / day.
- Consume 1,200 mg per day of dietary calcium. (The risk of developing a recurrent stone on the normal calcium diet was 51% lower than on the lower calcium diet. Supplemental calcium, in contrast, may be associated with an increased risk of stone formation.)
- Increase fruit and vegetable intake.
- Reduce intake of high-acid foods like aerated drinks, oil and butter.
- Increase dietary citrate intake: Lemon, oranges, grapefruit juice.
- Limit non-dairy animal protein.
| Food | Serving Size | Average Calcium Content (mg) | Estimated Absorption (%) | Calcium Absorbed (mg) |
|---|---|---|---|---|
| Milk or yoghurt (Whole, 2%, 1%, skim) | 250ml | 300 | 32 | 96 |
| Brocoli | 125ml | 35 | 61 | 22 |
| Spinach | 125ml | 115 | 5 | 6 |
| Almonds | 125ml | 206 | 21 | 43 |
Oranges, kiwi, Figs, Sesame are also good sources of calcium
Urine alkalinization Medical treatment depends upon the type of stone. It does not dissolve any existent stone but may reduce the chances of reformation
- The mainstay for medical management of uric acid stones is alkalinization (increasing the pH) of the urine.
- Acetazolamide (Diamox) is a medication that alkalinizes the urine.
- Dietary supplements are available that produce a similar alkalinization of the urine. These include sodium bicarbonate, potassium citrate, magnesium citrate. Aside from alkalinization of the urine, these supplements have the added advantage of increasing the urinary citrate level,which helps to reduce the aggregation of calcium oxalate stones.
One of the recognized medical therapies for prevention of stones is the thiazide and thiazide-like diuretics, such as chlorthalidone or indapamide. These drugs inhibit the formation of calcium-containing stones by reducing urinary calcium excretion. Sodium restriction is necessary for clinical effect of thiazides, as sodium excess promotes calcium excretion.
For people with hyperuricosuria and calcium stones, allopurinol is one of the few treatments that have been shown to reduce kidney stone recurrences. Allopurinol interferes with the production of uric acid in the liver. The drug is also used in people with gout or hyperuricemia (high serum uric acid levels).